Adult-onset neurological disorders panel
In the National Genomic Test Directory, a number of gene panels applicable to adult neurodegenerative disease indications have been combined, creating an adult-onset neurological disease ‘super panel’.
Overview
The adult-onset neurological disorders panel will be applied to all whole genome sequencing (WGS) requests in adults with neurodegenerative conditions for the test directory indications listed in the next section. This includes inherited dementia, motor neurone disease (also known as amyotrophic lateral sclerosis) and movement conditions.
Clinical application
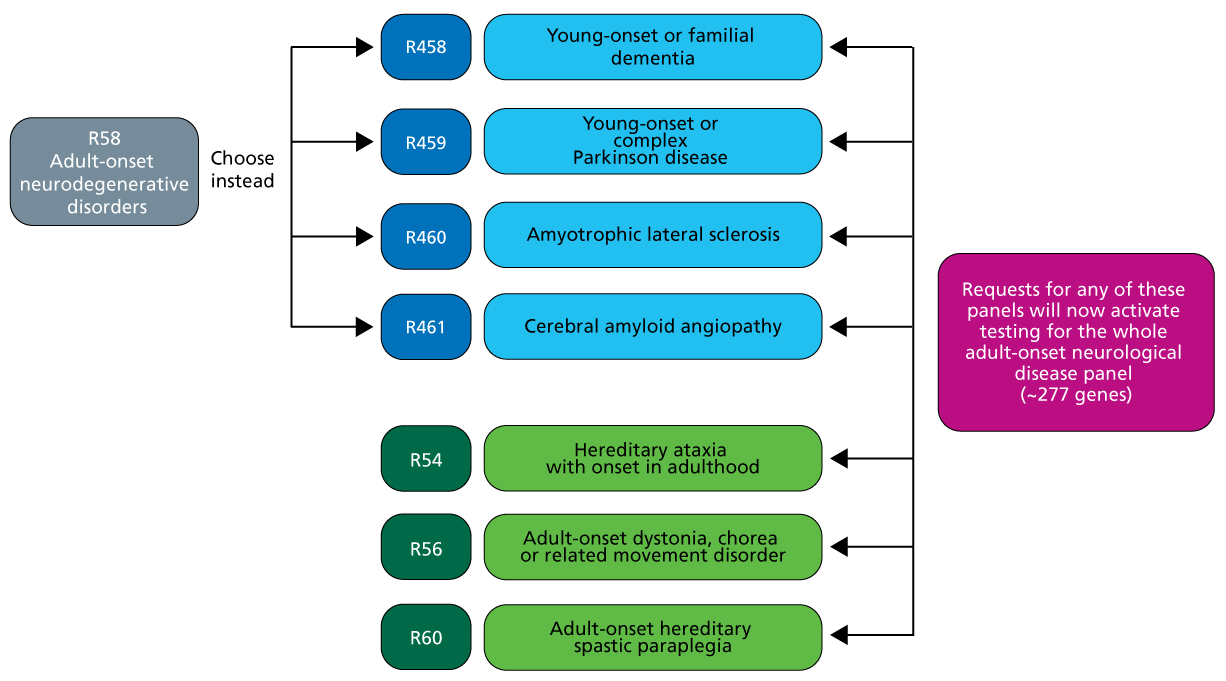
All genes on the following panels are included in the adult-onset neurological disease ‘super panel’:
- R54 Hereditary ataxia with onset in adulthood;
- R56 Adult onset dystonia, chorea or related movement disorder;
- R60 Adult onset hereditary spastic paraplegia; and
- Adult-onset neurodegenerative conditions: previously R58, this is now divided into individual indications:
- R458 Young onset or familial dementia;
- R459 Young onset or complex Parkinson disease;
- R460 Amyotrophic lateral sclerosis; and
- R461 Cerebral amyloid angiopathy.
Any request for a panel in the list above will activate testing for the entire adult-onset neurological disorders panel.
Figure 1: Movement and neurodegenerative disease gene panels included in the adult-onset neurological disorders panel (relevant from April 2026)
Single gene testing remains available for some indications also covered by this panel – for example, R68 Huntington disease and R337 CADASIL. In patients in whom one of these conditions is highly likely to be the correct diagnosis, this testing should be requested prior to WGS. For more information about testing, see Clinical suspicion of Huntington disease and Patient with suspected cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
Other overlapping panels can be considered at the time of WGS referral, including:
- R62 Adult onset leukodystrophy;
- R78 Hereditary neuropathy or pain disorder; and
- childhood-onset gene panels for patients with early onset symptoms:
- R55 Hereditary ataxia with onset in childhood
- R57 Childhood onset dystonia, chorea or related movement disorder
- R61 Childhood onset hereditary spastic paraplegia; and
- R109 Childhood onset leukodystrophy.
Patients with epilepsy or leukodystrophy as a core aspect of their neurodegenerative diagnosis may be eligible for additional testing. For more information, please see Adult with epilepsy likely to be genetic in origin and Adult with suspected inherited white matter disorder.
Note that the above lists are not exhaustive. It is recommended that all relevant panels are requested at the point of testing for the purposes of variant interpretation.
The adult-onset neurological disorders panel test is undertaken using WGS. Additional confirmatory testing is conducted where required for variant interpretation.
Short tandem repeat (STR) testing is included within WGS analysis for relevant panels and does not need to be requested separately. For example, testing for spinocerebellar ataxia (types 1, 2, 3, 6, 7, 10, 12 and 17) and Friedreich ataxia is included in the R60 Adult onset hereditary spastic paraplegia indication, and will therefore be included in analysis for the adult-onset neurological disorders panel.
A full list of included STRs is available from local Genomic Laboratory Hubs (GLHs). Please note that RFC1 STR testing will only be included in patients with relevant clinical features and where it has been specifically indicated on the request form.
Possible outcomes of the adult-onset neurological disorders panel
The adult-onset neurological disorders panel may find a genetic cause for the patient’s symptoms. A diagnosis may, in turn, affect treatment and broader management or surveillance of the condition; it could also provide important information for the wider family.
Alternatively, the test may find no genetic cause for the patient’s symptoms. This does not rule out a genetic condition; it simply means that, with the information we have about genomics so far, there is no genetic variant that can explain the patient’s symptoms.
Care should be taken during pre-test counselling to discuss all potential outcomes with the patient, including variants of uncertain significance and incidental findings.
Note that genetic variation associated with all modes of inheritance can be identified from testing under this indication. X-linked inheritance, autosomal dominant inheritance with reduced penetrance, mitochondrial inheritance with differing heteroplasmy and de novo variants should all be considered as possibilities within pre-test counselling.
If you are discussing genomics concepts with your patients, you may find it helpful to use the visual communication aids for genomics conversations.
Requesting the adult-onset neurological disorders panel
Patients with neurodegenerative conditions can have a wide range of clinical issues crossing the spectrum of neurological symptoms and signs. As such, genomic testing for likely neurogenetic conditions can identify changes in a number of genes with overlapping phenotypes, where more than one gene panel may be relevant. For example, variants in SPG11 are associated with a combined phenotype of spasticity, cerebellar ataxia, neuropathy and cognitive impairment.
Clinical questions about panel choice can be directed to your local GLH (and/or clinical genetics service).
Given this wide phenotypic spectrum, it is important that clear and comprehensive clinical information is included in the referral for testing. This can include any imaging findings and results of previous neurophysiological or genomic testing.
Other genomic testing, not always based on WGS, may be relevant. For information about testing for specific conditions or symptoms, check the GeNotes In the Clinic neurology pages. Some relevant examples include:
- Clinical suspicion of young-onset Parkinson disease;
- Patient with young-onset dementia;
- Patient with suspected cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL); and
- Adult with suspected inherited white matter disorder.
Where a specific condition has been considered, or where one has been ruled out based on other testing, this information should be included on the WGS test order form (see How to complete a test order form for WGS for support).
WGS is most effective when requested as a trio – that is, with samples from the affected individual and both parents. Particularly for younger adults, every effort should be made to include parents within the request, as this enables more efficient and effective variant interpretation and increases the likelihood of a positive finding. It is recognised that, for many adults with neurodegenerative conditions, involvement of parents may not be possible. As such, referral as a singleton is often appropriate.
Consent needs to be taken from the patient before any test requests can be made. A record of discussion form should be completed for each person being tested (so for trio testing, three forms would be needed) – see How to complete a record of discussion form for support. A consultee form signed by an appropriate relative or advocate should be obtained if an adult patient does not have capacity to consent to genomic testing.
Testing is also available for patients for whom a diagnosis is sought after death for the purpose of identifying support for a cause of death, confirmation of a diagnosis in an affected relative and counselling for relatives. It is recommended that testing in this scenario is discussed with the local Clinical Genetics service before going ahead.
Research
As part of the record of discussion, all families are asked if they agree to their samples being used anonymously in research. This is a personal decision for families, and they do not need to agree in order to access the test. Anonymous data is accessed by approved research groups (public and private) aiming to increase our understanding of the genome. There is a small chance that patients may be contacted by their clinicians in the future with a diagnosis, or information about a trial, due to findings made in the research setting.
Key messages
- The National Genomic Test Directory adult-onset neurological disorders panel is a whole genome sequencing (WGS) test that combines a number of gene panels applicable to adult neurodegenerative disease into one ‘super panel’.
- Any WGS requests for any of the individual panels will activate testing for the entire adult-onset neurological disorders panel – including inherited dementia, motor neurone disease and movement disorders.
- Short tandem repeat (STR) testing is included within WGS analysis for relevant panels and does not need to be requested separately.
Resources
For clinicians
- NHS England: National Genomic Test Directory