Coarctation of the aorta
Coarctation of the aorta is a narrowing of the aorta, usually distal to the origin of the left subclavian artery and close to the ductus arteriosus. It narrows the lumen of the aorta and causes hypertension in the upper body and hypoperfusion in the lower body. It may be seen alongside other congenital heart defects, such as bicuspid aortic valve.
Overview
Coarctation of the aorta can be diagnosed antenatally through ultrasound scanning. Antenatal diagnosis can be challenging, and clinical features after birth may be mild, non-specific or less problematic until the child is older. When there is suspicion of a cardiac anomaly, a referral should be made to a specialist paediatric cardiology service for assessment and management.
Figure 1 indicates the anatomical change in coarctation of the aorta.
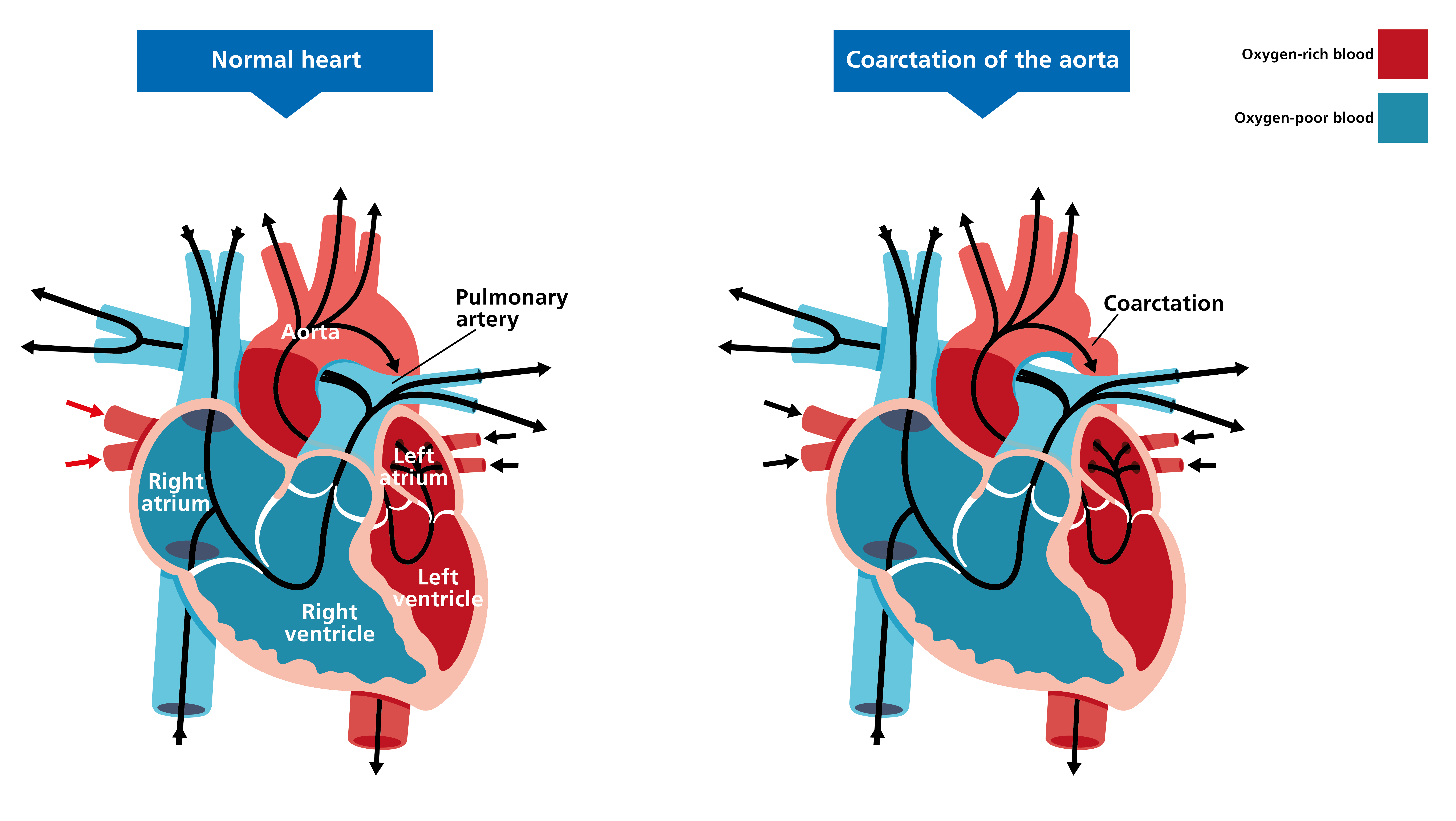
Figure 1: Coarctation of the aorta
Clinical features
Clinical features of coarctation of the aorta will depend on how severe the coarctation is and how much blood flow is possible around the body. They may include:
- poor feeding;
- lethargy;
- tachypnoea;
- congestive heart failure; and
- differences between the upper and lower limbs, such as:
-
- delayed pulse in the lower limbs (radiofemoral delay);
- blood pressure discrepancies between the upper and lower limbs (for example, the upper limbs might experience hypertension while the lower limbs experience hypotension or normal blood pressure);
- skin of the upper body appearing pink in colour, while the lower body is cyanotic; and
- heart murmur, specifically a systolic murmur in the left infraclavicular area. If patients present later in life, it is often with a systolic or continuous murmur or hypertension.
Genomics
The majority of cases are not associated with an identified genetic cause. However, because some will be linked to underlying Turner syndrome, genomic testing should still be considered.
Chromosomal tests using a karyotype and/or microarray are recommended for congenital heart disease.
Inheritance and genomic counselling
The recurrence risk following an affected pregnancy is around 1 in 200 (or 0.5%). Where a congenital heart anomaly is detected, there is a 1% chance of having a further pregnancy or child with congenital heart disease (which may be a different form of congenital heart disease to that of the previous child).
Parents who have a child diagnosed with Turner syndrome have a slightly greater recurrence risk (just over 1%) of having a further pregnancy with the condition.
Management
If the baby has a severe form of coarctation of the aorta, surgery will be offered in the first few days of life and several techniques may be used:
- removing the narrowed section of the aorta and anastomosing the two ends;
- balloon angioplasty or stenting; and
- surgical angioplasty with grafts.
Diuretics and inotropes are used to treat congestive heart failure, if it occurs.
Any child also confirmed to have Turner syndrome should be managed according to national guidance.
For parents with a child diagnosed with Turner syndrome or a complex congenital heart anomaly, a fetal echocardiogram should be offered during any future pregnancies, depending on local protocols.
Resources
For clinicians
- MedlinePlus: Coarctation of the aorta
- NHS England: National Genomic Test Directory
- The Fetal Medicine Foundation: Ultrasound demonstration coarctation of the aorta
For patients
- British Heart Foundation: Understanding your child’s heart: Coarctation of the aorta (PDF, 19 pages)
- Great Ormond Street Hospital for Children NHS Foundation Trust: Information for families: Coarctation of the aorta (PDF, three pages)
- Turner Syndrome Support Society