Long QT syndrome
Long QT syndrome is characterised by QT prolongation on an electrocardiogram. It is associated with ventricular arrhythmias and sudden death, most commonly triggered by adrenergic activation.
Overview
Long QT syndrome (LQTS) is a channelopathy that can cause collapse and life-threatening arrhythmia through its prolongation of a fixed electrical interval (the QT interval), resulting in a vulnerable period that can then predispose to ventricular arrhythmia. The presentation of LQTS is variable: some individuals are asymptomatic, while others present with a variety of symptoms that can include palpitations, dizziness and/or syncope and, more rarely, cardiac arrest or sudden death. A prolonged QT interval on electrocardiogram (ECG) can be an acquired phenomenon through a number of mechanisms, which is why diagnosis must exclude inherited non-inherited causes such as electrolyte disturbance. In its inherited form, LQTS has been linked to variants in a small number of genes, with the majority following a pattern of autosomal dominant inheritance.
Clinical features
- Individuals affected by LQTS may be asymptomatic, or may experience palpitations, dizziness and/or syncope. The first presentation may be cardiac arrest or sudden cardiac death.
- Onset of puberty is associated with an increased symptom burden, and there are well-recognised risk variances between genders depending on age and genetic subtype.
- In LQTS type 1, arrhythmias are associated with events that result in elevated sympathetic activity and adrenergic drive, such as intense exercise and emotional stress (for example, swimming and diving).
- In LQTS type 2, auditory stimuli are a recognised trigger, and the postpartum period is a time of elevated risk.
- In patients with LQTS type 3, events tend to occur during rest or sleep, when the QT interval is prolonged at slower heart rates.
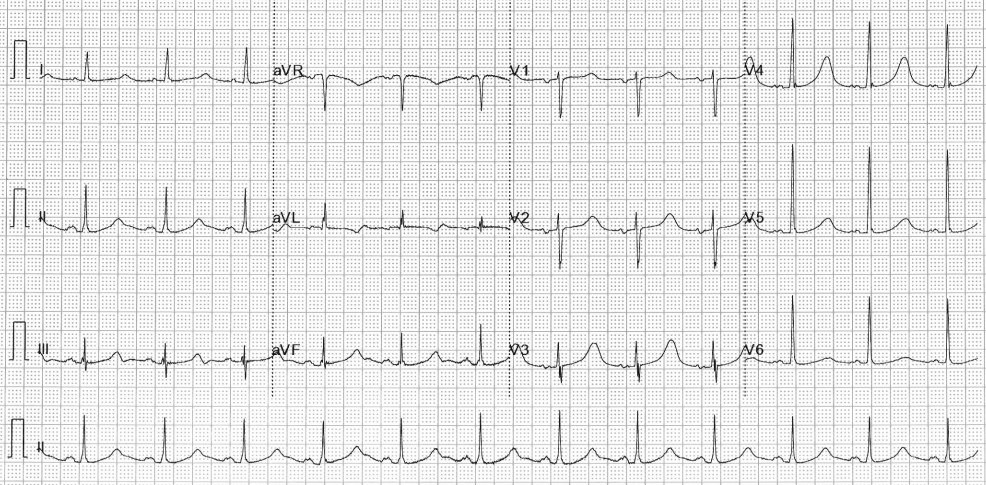
Figure 1: ECG demonstrating QT prolongation in a patient with Jervell and Lange-Nielson syndrome
Genomics
- There are numerous subtypes of LQTS, defined by the associated gene – though variation in phenotypic presentation is well recognised.
- Depending on the quality of the clinical phenotypic, genetic yield is in the region of 60%.
- The vast majority of those genetically diagnosed have a variant in one of the three most commonly associated LQTS genes: KCNQ1 (LQTS type 1), KCNH2 (LQTS type 2) and SCN5A (LQTS type 3). It is thought that these genes account for over 90% of the variants seen with an autosomal dominant pattern of inheritance.
- Penetrance is high, though expression can vary between individuals.
- Some subtypes of LQTS are associated with very specific and malignant phenotypes. Examples include:
- Andersen-Tawil syndrome (caused by variants in KCNJ2, inherited in an autosomal dominant pattern), also known as LQTS type 7, which is associated with a prolonged QT interval, frequent (often bidirectional) ventricular arrhythmias, periodic paralysis and dysmorphic facial features;
- Timothy syndrome (caused by variants in CACNA1C, inherited in an autosomal dominant pattern), also known as LQTS type 8, which is associated with syndactyly, specific facial features such as micrognathia, immunodeficiency, congenital heart disease and neurodevelopment delay); and
- Jervell and Lange-Nielson syndrome (caused by biallelic variants in KCNQ1 or KCNE1, inherited in an autosomal recessive pattern), in which QT prolongation is associated with sensorineural hearing loss and the QT interval tends to be particularly prolonged, with a higher risk of arrhythmias.
Figure 2: The genotype-phenotype relationship for long QT syndrome types 1, 2 and 3
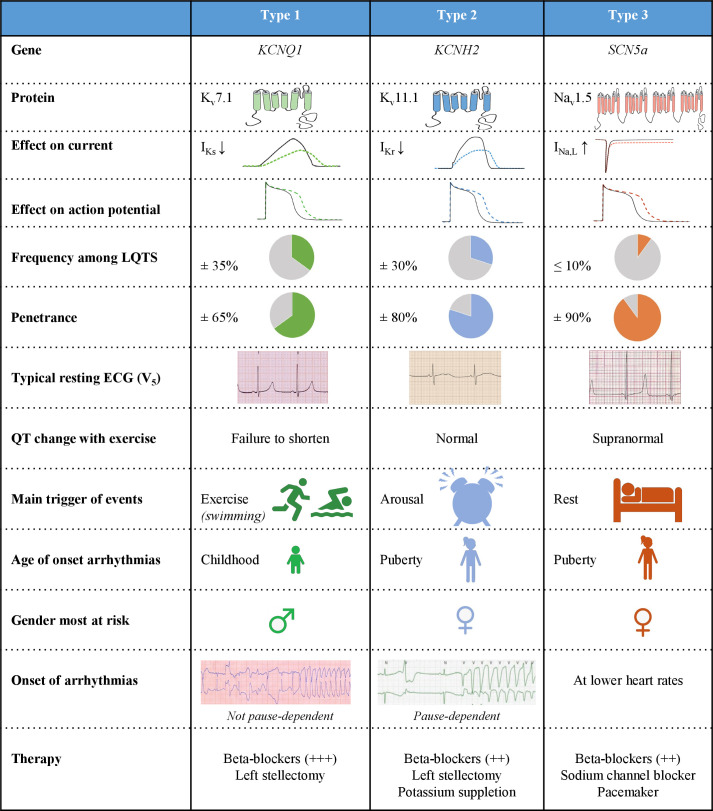
Reproduced under Creative Commons Attribution 4.0. Originally published by Heart 2022 (see references list below).
Inheritance and genetic counselling
- LQTS is most commonly inherited as an autosomal dominant condition.
- Individuals affected by an autosomal dominant condition have one working copy of the gene, and one with a pathogenic variant.
- The chance of a child inheriting the gene with the variant from an affected parent is 1 in 2 (50%).
- Incomplete penetrance can occur (that is, not everyone who has the variant develops the disease).
- Recessive forms of the condition have also been reported.
- If both parents are carriers of an autosomal recessive condition, with each pregnancy there is a:
- 1-in-4 (25%) chance of a child inheriting both gene copies with the pathogenic variant and therefore being affected;
- 1-in-2 (50%) chance of a child inheriting one copy of the gene with the pathogenic variant and one normal copy, and therefore being a healthy carrier themselves; and
- 1-in-4 (25%) chance of a child inheriting both normal copies and being neither affected nor a carrier.
- If both parents are carriers of an autosomal recessive condition, with each pregnancy there is a:
- Taking a three-generation family history, as well as identifying any previously known familial pathogenic or likely pathogenic variants, is an essential part of genetic counselling for LQTS.
- There is variability between individuals and within families, likely due to the presence of ‘modifier’ genes that increase or decrease the impact of a pathogenic or likely pathogenic variants, as well as ‘silent mutation carriers’, which result in the variation seen in phenotypic expression.
- If you are discussing genomics concepts with your patients, you may find it helpful to use the visual communication aids for genomics conversations.
Management
- All patients with LQTS should be given lifestyle advice.
- Certain drugs may increase the likelihood of arrhythmia in the setting of LQTS, and patients should be directed to CredibleMeds for a list of drugs to avoid.
- During gastrointestinal illness, affected individuals should keep well hydrated using oral rehydration therapy (such as Dioralyte) with a low threshold for attending hospital.
- Affected individuals should avoid gene-specific triggers (such as cold water swimming and diving).
- The mainstay of treatment is beta blockade (ideally non-selective beta blockers such as nadolol and propranolol).
- Mexiletine is useful in patients with LQTS type 3, who tend to be bradycardic.
- Other anti-arrhythmias such as Flecainide can be considered in specific LQTS subtypes under expert guidance.
- Implantable cardioverter-defibrillator (ICD) implantation is recommended in individuals who have survived cardiac arrest, or have arrhythmic syncope or haemodynamically unstable ventricular arrhythmia despite optimal beta blockade.
- This may be done in combination with left sympathetic cardiac denervation (LSCD). It may also be considered in isolation, in those for whom ICD is not appropriate and adrenergic stimulus has been demonstrated to be a mechanism for symptoms, such as small paediatric patients.
- ICD implantation or LCSD should be considered in patients with symptomatic LQTS where beta-blockers and genotype-specific therapies are not tolerated or are contraindicated at the therapeutic dose.
Resources
For clinicians
- NHS England: National Genomic Test Directory
References:
- Schwartz PJ, Crotti L and Insolia R. ‘Long-QT syndrome: From genetics to management‘. Circulation: Arrhythmia and Electrophysiology 2012: volume 5, issue 4, pages 868–77. DOI: 10.1161/CIRCEP.111.962019
- Wilde AAM, Amin AS and Postema PG. ‘Diagnosis, management and therapeutic strategies for congenital long QT syndrome‘. Heart 2022: volume 108, issue 5, pages 332–338. DOI: 10.1136/heartjnl-2020-318259
- Wilde AAM, Semsarian C, Márquez MF and others. ‘European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus Statement on the state of genetic testing for cardiac diseases‘. EP Europace 2022: volume 24, issue 8, pages 1,307–1,367. DOI: 10.1093/europace/euac030
- Zeppenfeld K, Tfelt-Hansen J, de Riva M and others. ‘2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden death of the European Society of Cardiology (ESC) endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC)‘. European Heart Journal 2022: volume 43, issue 40, pages 3,997–4,126. DOI: 10.1093/eurheartj/ehac262
For patients
- British Heart Foundation: Long QT syndrome
- Cardiac Risk in the Young
- CredibleMeds
- NHS Health A to Z: Long QT syndrome