Brugada syndrome
Brugada syndrome is an inherited arrhythmia condition that may manifest as syncope or sudden death (often during sleep) secondary to ventricular fibrillation in patients with a structurally normal heart.
Overview
Brugada syndrome is a channelopathy which can cause ventricular arrhythmia. The presentation is variable: many individuals are asymptomatic, but others may present with symptoms including palpitations, syncope and, rarely, cardiac arrest/sudden death. In many individuals, the genetic cause of the condition is not found. In those with a pathogenic variant identified, SCN5A is the most common gene. The inheritance of Brugada syndrome usually follows an autosomal dominant pattern.
Clinical features
- Clinical features of Brugada syndrome include palpitations, syncope and sudden death. The majority of affected individuals are asymptomatic.
- The first presentation of Brugada syndrome is commonly around 40 years of age. It is more prevalent in males of South East Asian ethnicity.
- Triggers for ventricular arrhythmia include fever, dehydration, certain medications, heavy alcohol consumption and cocaine use.
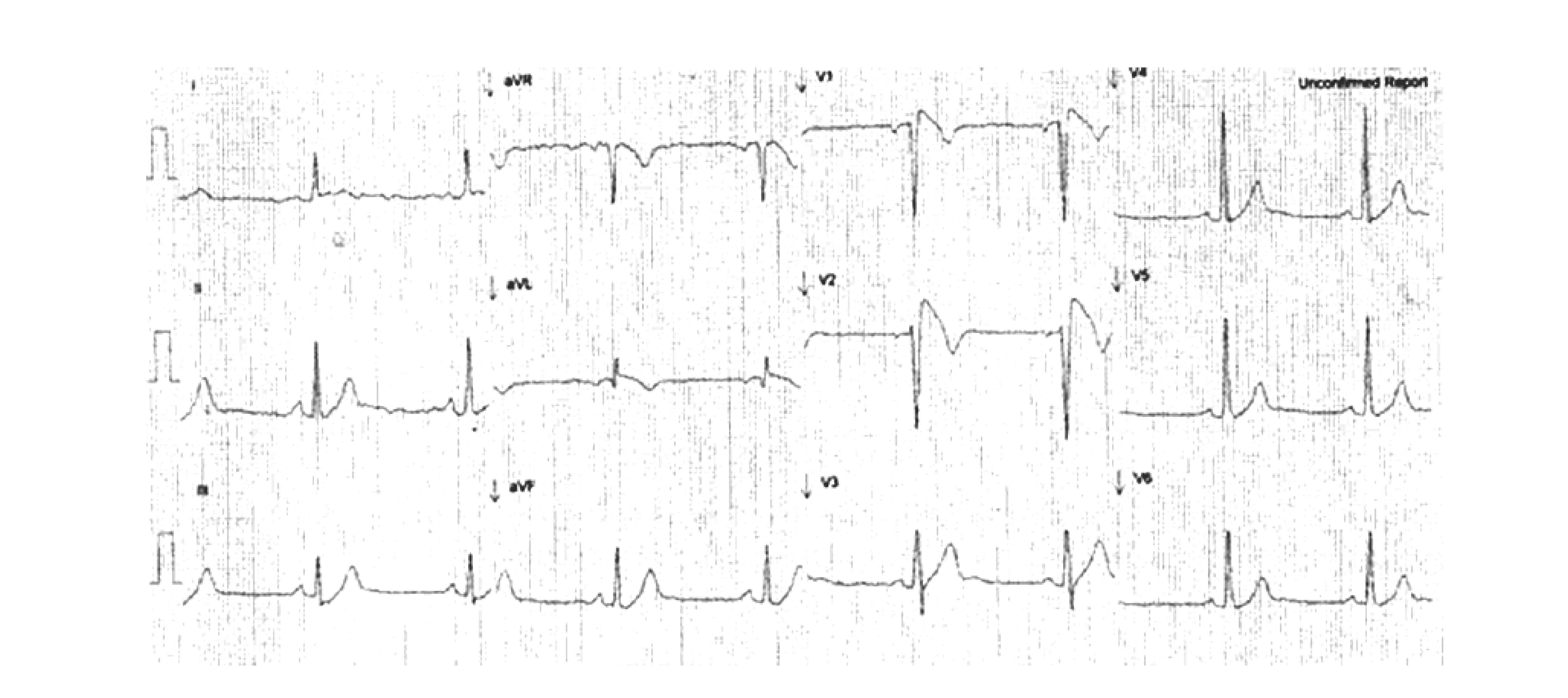
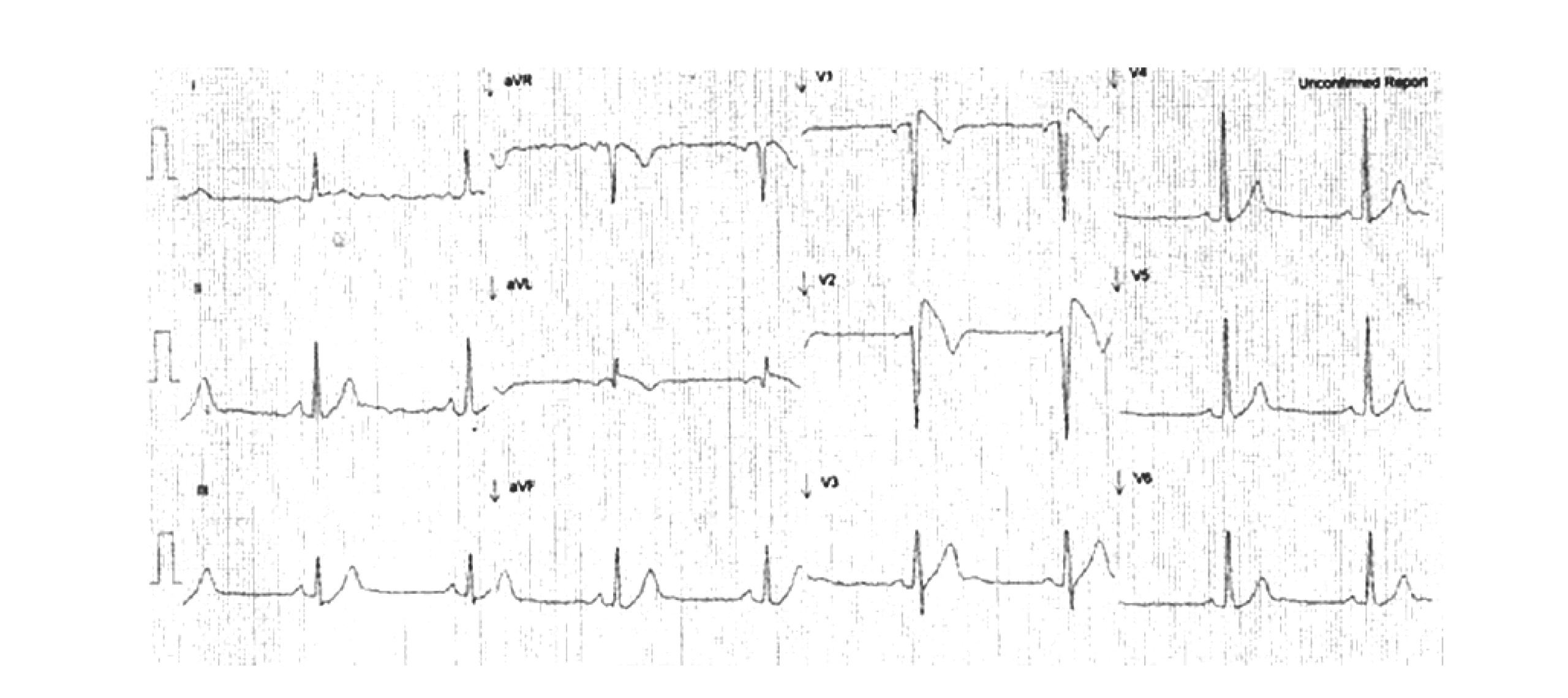
Figure 1: ECG demonstrating the type 1 Brugada ECG pattern in standard leads V1 and V2
Genomics
- Most patients with Brugada syndrome are not found to have a monogenic disease-causing variant. However, up to 20% of affected individuals have a pathogenic variant in the SCN5A gene, which encodes a subunit of the cardiac sodium channel responsible for regulating rapid sodium current in the heart.
- Pathogenic SCN5A variants are also associated with long QT syndrome type 3 and progressive cardiac conduction disease. Patients may describe some relatives with Brugada syndrome and others with different phenotypes; this suggests the existence of overlap syndromes (that is, some family members experience different clinical manifestations caused by the same genotype).
Diagnosis
The diagnosis of Brugada syndrome requires demonstration of a type 1 Brugada ECG pattern. The Brugada type 1 pattern (see figure 1 below) is an ECG finding of ‘coved’ ST segment elevation >0.2mV with T wave inversion in at least one right precordial lead (V1–V2) in the second, third or fourth intercostal spaces. Standard ECG lead positions refer to V1–V2 in the fourth intercostal spaces; high ECG lead positions refer to V1–V2 in the second or third intercostal spaces.
Figure 1: ECG demonstrating the type 1 Brugada ECG pattern in standard leads V1 and V2
When the Brugada type 1 ECG pattern is seen at rest (spontaneous type 1 Brugada ECG pattern), a Brugada syndrome diagnosis can be made. When the Brugada type 1 ECG pattern occurs with intercurrent fever or following administration of an intravenous sodium channel blocker such as ajmaline (inducible type 1 Brugada ECG pattern), other clinical features, such as ventricular fibrillation, arrhythmic syncope or relevant family history, are required to make the diagnosis.
In the case of sudden death, diagnosis may be made via molecular autopsy. A molecular diagnosis can be made if genomic testing identifies a pathogenic variant in a Brugada syndrome-linked gene which aligns with the clinical presentation. For information about testing, see Adult with Brugada syndrome or Sudden unexplained death or survivor of a cardiac arrest or Sudden death in a child under 18 years of age.
Inheritance and genomic counselling
- Most of the pathogenic variants associated with Brugada syndrome are inherited in an autosomal dominant pattern, but they can also arise de novo.
- Individuals affected by an autosomal dominant condition have one working copy of the gene, and one with a pathogenic variant.
- The chance of a child inheriting the gene with the variant from an affected parent is 1 in 2 (50%).
- Incomplete penetrance can occur (that is, not everyone who has the variant develops the disease).
- Although pathogenic variants are inherited equally by men and women, the phenotype appears to affect men more frequently.
- Research suggests that variants in genes other than SCN5A are also important in disease expression, following a polygenic mode of inheritance in some families. Genomic testing via the National Genomic Test Directory supports testing a small panel of genes, including SCN5A.
- All first-degree relatives of an individual with Brugada syndrome should be offered clinical screening in combination with genomic testing where appropriate. It is important that this is undertaken in a specialist inherited cardiac conditions clinic due to the complexity of the inheritance pattern.
- If you are discussing genomics concepts with your patients, you may find it helpful to use the visual communication aids for genomics conversations.
Management
- The mainstay of treatment in Brugada syndrome is careful lifestyle advice.
- Certain drugs may increase the likelihood of arrhythmia in the setting of Brugada syndrome. Patients should be directed to BrugadaDrugs.org for the list of drugs to avoid.
- Affected individuals should be given advice regarding prompt treatment of fever with antipyretics (such as paracetamol and ibuprofen) due to increased risk of arrhythmia.
- During a diarrhoea and vomiting illness, affected individuals should keep well hydrated using oral rehydration therapy (such as Dioralyte).
- Affected individuals should be advised to avoid excessive alcohol consumption, cocaine and cannabis use and eating large meals before bed due to increased risk of arrhythmia.
- Implantable cardioverter-defibrillator (ICD) implantation is recommended in individuals who have survived cardiac arrest or have documented episodes of spontaneous ventricular arrhythmia.
- ICD implantation should be considered in individuals with a spontaneous type 1 Brugada ECG pattern and syncope.
- Asymptomatic affected individuals may undergo electrophysiology studies to assess whether there is inducible ventricular tachycardia or ventricular fibrillation.
- Affected individuals with recurrent ventricular arrhythmias may be treated using medication (such as quinidine) or with catheter ablation.
- Individuals with Brugada syndrome should be considered for genomic counselling (see the test directory for eligibility criteria).
Resources
For clinicians
- National Organization for Rare Disorders: Brugada syndrome
- NHS England: National Genomic Test Directory
References:
- Zeppenfeld K, Tfelt-Hansen J, de Riva M and others. ‘2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden death of the European Society of Cardiology (ESC) endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC)‘. European Heart Journal 2022: volume 43, issue 40, pages 3,997–4,126. DOI: 10.1093/eurheartj/ehac262
For patients
- British Heart Foundation: Brugada syndrome
- BrugadaDrugs.org
- Cardiac Risk in the Young
- NHS Health A to Z: Brugada syndrome