Transposition of the great arteries
Transposition of the great arteries is a congenital heart anomaly that usually requires surgery within the first few weeks of life.
Overview
In transposition of the great arteries (TGA), the position of the two main arteries carrying blood out of the heart are switched: the pulmonary artery is joined to the left ventricle, and the aorta to the right ventricle. The condition can be diagnosed during ultrasound in both the antenatal and postnatal period. It is incompatible with life without a shunt to allow blood mixing (such as a patent ductus arteriosus or a ventricular septal defect). Most cases are of unknown cause.
Clinical features
Clinical features of TGA are:
- rapid breathing or problems with breathing;
- weak pulse;
- blue or purple tint to lips and/or skin (cyanosis);
- difficulty feeding;
- poor appetite; and
- inadequate weight gain.
For comparison with a normal heart, see figure 1.
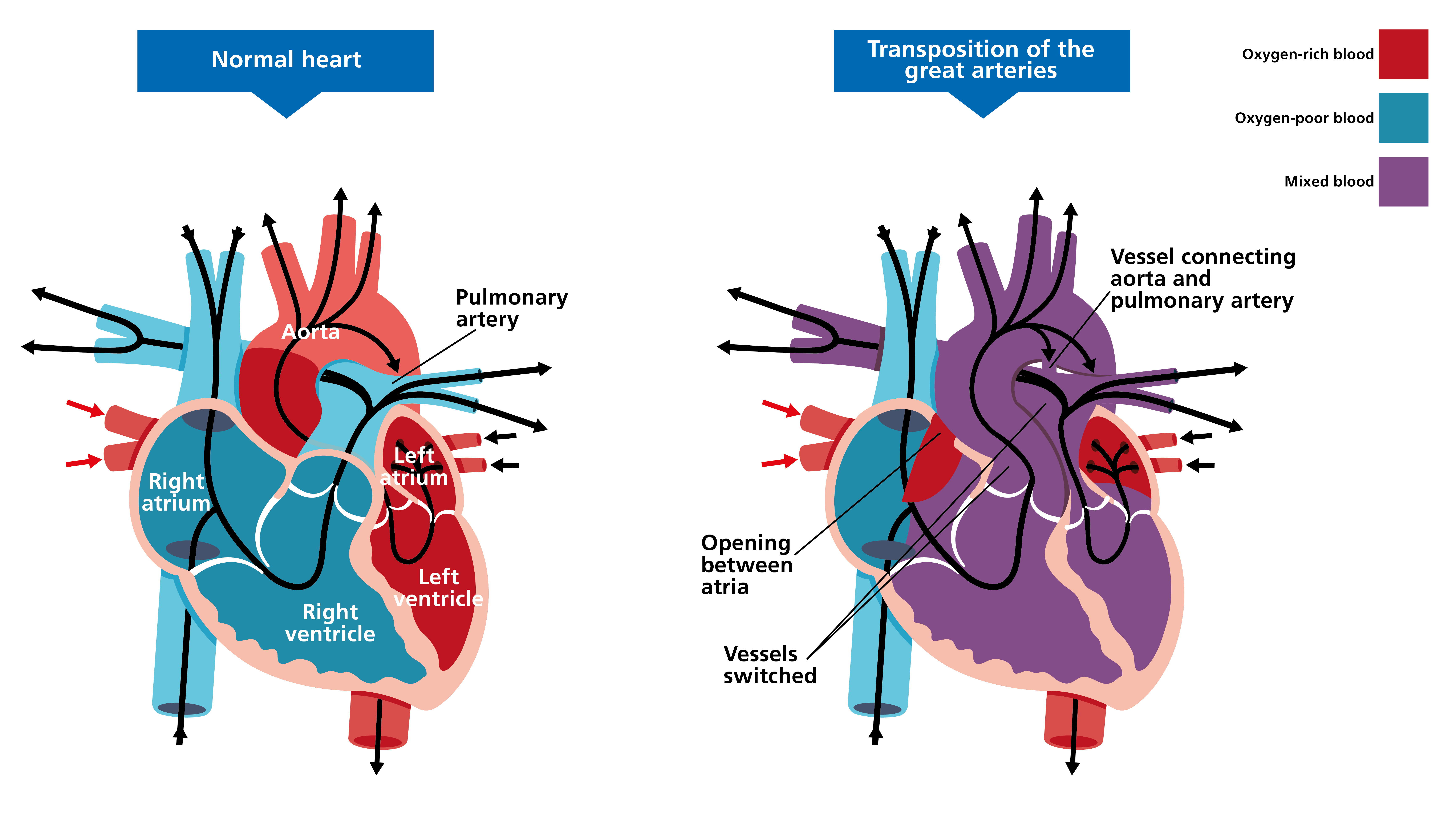
Figure 1: Transposition of the great arteries
This video shows how TGA works (shared with kind permission from Leeds Congenital Hearts).
Genomics
Most of the time, TGA occurs on its own; however, it can occur with other cardiac symptoms, such as a ventricular septal anomaly.
Because the cause of TGA is often unknown, there are no commonly associated genetic variants. Where TGA is associated with other anomalies detected either during ultrasound or postnatally (such as ciliopathy and heterotaxy conditions), a genomic test may be warranted. The type of test would be determined following full assessment and consultation.
Diagnosis
TGA may be diagnosed either prenatally on ultrasound scan, or postnatally through a combination of examination findings and echocardiography.
For information about genomic testing for TGA when associated with other anomalies, see:
Inheritance and genomic counselling
TGA is considered to be associated only rarely with genetic conditions and to have a low risk of recurrence among relatives of affected patients.
Management
Most babies will be given prostaglandin quickly after birth to allow blood to circulate more effectively. A balloon septostomy will be performed in most cases to ensure adequate oxygenation while awaiting surgery. Surgery, during which the major arteries are switched to the normal position, is usually performed within the first three weeks of life.
Resources
For clinicians
- American Heart Association: Transposition of the Great Arteries
- Great Ormond Street Hospital for Children NHS Foundation Trust: Transposition of the great arteries
- NHS England: National Genomic Test Directory
References:
- Blue GM, Mekel M, Das D and others. ‘Whole genome sequencing in transposition of the great arteries and associations with clinically relevant heart, brain and laterality genes‘. American Heart Journal 2022: volume 244, pages 1–13. DOI: 10.1016/j.ahj.2021.10.185
For patients
- British Heart Foundation: Understanding your child’s heart: Transposition of the great arteries (PDF, 24 pages)
- Tiny Tickers